Nitric Oxide can cause health problems. However, it has also been approved for use at doses of inhalation gas for NEW BORN Babies at 40ppm for Pulmonary Vasodilation. Frankly I think we have little to worry about as even 200ppm Sodium Nitrite in 1Gallon of Brine is very Dilute and will make nowhere near the FDA Approved 40ppm Nitric Acid Gas and definately not Clinical Toxicity of 80ppm!
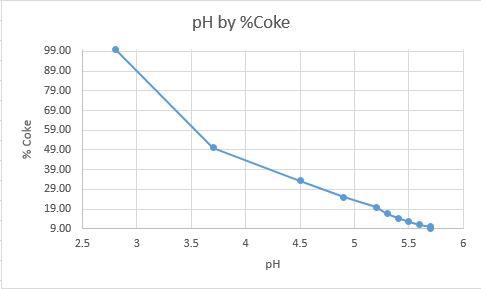
Now it has been 30 years since my Advanced Chemistry Class and have no desire to do the math to find the Exact amount of Gas that will be generated from 200ppm Nitrite in 3785.41g of water and adding 354.88g Cola at a pH of 2.52...
Just an educated wild ass guess...While adding Cola or Acid of any kind to 100 or 1000 gallons of Curing Brine in an insufficiently ventilated, 120sqft Cold Room used to inject Hams, May be a Very Bad Idea! I highly doubt there is anything to worry about, Nitric Acid wise, adding Cola to ONE Gallon of Pops Brine.
Now getting back to Acid or Cola inactivating Sodium Nitrite? That is enough reason to not do it! The rest is arguing a moot point, Unless there are any Chemists here, who can show a TOXIC amount of Nitric Oxide, 80ppm, will come from 1 Gallon of 200ppm Brine...JJ
Taken from a Trusted Medical Journal...
http://toxsci.oxfordjournals.org/content/59/1/5.full
[h3]Pulmonary Vasodilation[/h3]
The primary demonstrated clinical indication for inhaled nitric oxide is hypoxic respiratory failure associated with persistent pulmonary hypertension of the newborn (PPHN). In 1992, Roberts
et al. and Kinsella
et al. reported that inhaled nitric oxide produced rapid and significant increases in oxygenation in term and near-term infants with PPHN, without detectable toxicity. In late 1999, positive findings in several randomized clinical trials led the Food and Drug Administration to approve inhaled nitric oxide for open-label use in these patients (
Davidson et al., 1998;
Day et al., 1996;
The Neonatal Inhaled Nitric Oxide Study Group, 1997;
Roberts et al., 1997;
Wessel et al., 1997). A recent meta-analysis has also confirmed the clinical efficacy of inhaled nitric oxide for the treatment of PPHN (
Finer and Barrington, 2000). Low doses of inhaled nitric oxide have been reported to be clinically effective, and most current dosing recommendations do not exceed 40 ppm. At this dose, there is little measurable short-term toxicity. Indeed, it is noteworthy that in the large randomized trials of inhaled nitric oxide, major clinical toxicity (e.g., methemoglobinemia) was observed only at doses ≥ 80 ppm (
Davidson et al., 1998;
Wessel et al., 1997). However, even low doses of inhaled nitric oxide may exert toxicity at the cellular level, potentially leading to long-term pulmonary complications. In this regard, nitrotyrosine residues have been detected in the lungs after 10 days of life in 2 of 12 infants who required prolonged ventilation and were treated with nitric oxide (up to 20 ppm) for 1–4 days (
Hallman et al., 1998). These findings suggest that endogenous nitric oxide can alter proteins in the lung. Adverse outcomes have also been observed at clinical doses during weaning from nitric oxide, since rapid withdrawal can result in severe rebound pulmonary vasospasm (
Atz et al., 1996;
Cueto et al., 1997).